
Ms. N is a 23-year-old woman who comes to see you complaining of a rash.
Ms. N complains of frequent “breakouts” on her face for the last several years. She reports the use of many topical over-the-counter agents over the years. She complains of feeling greasy and the need to “squeeze pus” out of lesions on a regular basis.
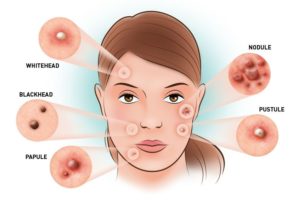
On examination, over the forehead, cheeks, and chin there are many erythematous papules, occasional pustules, and open and closed comedones. There is a predominance of larger nodules along the jaw line. Similar erythematous papules involve the upper back and chest. There is neither significant background erythema nor scaling in the scalp, eyebrows, or nasolabial folds. Figure 29-2 shows her on her initial visit.
The patient is in good health and is not overweight. She is not taking any oral medications. She reports regular menstrual cycles and notes that the breakouts are worse around the time of her period. She does not report easy flushing or any increased hair growth on the face or chest. She has 1 healthy child.
A management plan was discussed with the patient, including an appropriate skin care regimen, appropriate product selection, and use of systemic and topical medications. At follow-up in 3 months, the patient had significantly fewer active lesions with evidence of dyspigmentation associated with resolving lesions.
S:23- year old woman who complains of rash and breakouts for the last several years, seeks treatment now for regularly feeling greasy and the needing to “squeeze pus” out of lesions. Breakouts worsen around the time of her period. She does not report easy flushing, hair growth on the face or chest. She has used many topical over-the-counter agents over the years.
O: Skin:Erythematous papules, few pustules and open and closed comedones on the forehead, cheeks and chin. Large predominate nodules on the jaw line. Erythemayous papules on the chest and back.
Scalp/ eyebrows/ nasolabial folds: unremarkable, no significant background erythema, or scaling
A: Chronic acne vulgaris
Rosacea
Perioral dermatitis
P: Counseling and management plan was discussed on appropriate skin care regimen, product selection and use of systemic and topical medications.
Summary: Diagnosing rashes should be based on the morphology of the lesion, then the distribution. Morphology is based on the primary lesion, which means typical element of eruption. Ms. N has 3 types of primary lesions papules, pustules and comedones. She has folliculopapular eruptions that affect the face, chest and upper back. Her primary lesions suggest acne as the primary diagnosis and top of the differential. Additionally, acne is a chronic course with intermittent flares, and Ms. S has had “break outs” for the past several years. Other folliculopapular conditions are also considered such as rosacea, which is a less likely differential because her symptoms lack background erythema and telangiectasias (spider veins). Perioral dermatitis is another differential, it presents with monomorphic small papules and is related to cosmetic, and topical steroid use. Mr. N presents with a mixture type of lesion, that include comedones, papules and nodules, and diffuse distribution. This presentation makes acne more likely and perioral dermatitis less likely. Usually acne vulgaris is seen in adolescence with chronic waxing and waning lesions. It is a highly prevalent condition and although it is most common during mid-to-late adolescence, acne may be persistent beyond, especially in women. Treatment involves reviewing general skin care techniques for acne prone skin. Things that aggravate the skin are vigorous scrubbing, abrasive cleaners, hair gels and other styling products. Medical therapy for acne is focused on decreasing sebum production, alternation of epithelial turnover and cohesiveness, and P acnesproliferation and accompanying inflammation. Other things to consider are oral contraceptives and spironolactone can be effective in adult women with recalcitrant (not responsive to treatment) acne.

This entry is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International license.